One Theory To Explain Them All? The Vagus Nerve Infection Hypothesis for Chronic Fatigue Syndrome
Big Theory
It could explain the Chronic Fatigue Initiatives pathogen study results. It could show how an infection could cause chronic fatigue syndrome, and then seemingly disappear. It integrates two of the biggest players in ME/CFS; the autonomic nervous system and the immune system. It focuses on the herpesviruses. It includes sensory nerves, an increasingly hot topic in ME/CFS/FM, and it follows an established model of fibromyalgia. It's the Vagus Nerve Infection Hypothesis (VNIH) for chronic fatigue syndrome, and it could change how this disorder is viewed, researched and treated.Created by Michael VanElzakker, a Tufts neuroscientist, the VNIH proposes that nerve loving viruses trigger a difficult to detect immune response which produces the fatigue and other symptoms present in chronic fatigue syndrome.
It's the Vagus Nerve Infection Hypothesis (VNIH) for chronic fatigue syndrome, and it could change how this disorder is viewed, researched and treated.Created by Michael VanElzakker, a Tufts neuroscientist, the VNIH proposes that nerve loving viruses trigger a difficult to detect immune response which produces the fatigue and other symptoms present in chronic fatigue syndrome.
Location, Location, Location
VanElzakker proposes that an infection triggers ME/CFS, but if his theory is right the most important thing about that infection is not what it is but where it is. That 'where' is the biggest nerve in the body; the vagus nerve - a 'wandering nerve' that stretches over much of our torso and sends its roots into most of the organs of the body.The vagus nerve isn't just any nerve; it's the nervous system's immune conduit to the brain. VE believes that an infection there doesn't need to be large to cause havoc in the brain; it just needs to be present.In some ways, vagus nerve appears, in fact, to be ripe for infection in ME/CFS. As it 'wanders' through the body it comes into contact with virus havens such as the esophagus, stomach, lungs and spleen, all of which have likely at one time or another harbored the herpesviruses (HHV6, HHV-5 [cytomegalovirus], HHV-4 [Epstein-Barr virus]) that have been thought to be associated with ME/CFS for decades.Most humans carry several of these herpesviruses in latent form unless some stressor or biological event allows them to become reactivated. VanElzakker believes that upon reactivation these viruses replicate and move outside the nerves where they run into glial cells that attempt to gobble them up. The glial cells perk up remarkably in the presence of viruses, releasing all manner of pro-inflammatory and neuroexcitatory compounds (proinflammatory cytokines [IL-1B, IL-6, TNF-a], glutamate, prostaglandins, nitric oxide and free radicals. )Receptors on the vagus nerve that sniff out these alarm signals tell the brain an infection is present, which then shuts the body down by sending out signals (fatigue, flu-like symptoms, pain, etc.) that slow the body down, tell it to stop moving, stop eating, stop thinking.Because these infections are localized right on the main immune conduit to the brain, VanElzakker believes they don't need to produce the outsized cytokine response researchers have been looking for. All they need to do is tweak the vagus nerve and let it and the brain the do the rest.You don't need a 'big' infection to produce ME/CFS; all you need is a little infection in the right place.
VanElzakker believes that upon reactivation these viruses replicate and move outside the nerves where they run into glial cells that attempt to gobble them up. The glial cells perk up remarkably in the presence of viruses, releasing all manner of pro-inflammatory and neuroexcitatory compounds (proinflammatory cytokines [IL-1B, IL-6, TNF-a], glutamate, prostaglandins, nitric oxide and free radicals. )Receptors on the vagus nerve that sniff out these alarm signals tell the brain an infection is present, which then shuts the body down by sending out signals (fatigue, flu-like symptoms, pain, etc.) that slow the body down, tell it to stop moving, stop eating, stop thinking.Because these infections are localized right on the main immune conduit to the brain, VanElzakker believes they don't need to produce the outsized cytokine response researchers have been looking for. All they need to do is tweak the vagus nerve and let it and the brain the do the rest.You don't need a 'big' infection to produce ME/CFS; all you need is a little infection in the right place.
The Key Component - Glial Cells
The glial cells that surround and protect the vagus nerve are the key. Once thought to be mere structural scaffolding for the nerves, these cells (e.g., astrocytes) are now known to regulate nervous system signaling, a fact that's been borne out in chronic fatigue syndrome's sister disease, fibromyalgia. Glial cell release of cytokines, glutamate, free radicals, etc. in the dorsal horn of the spinal cord causes increased pain sensitivity and allodynia in susceptible individuals. At some point the constant production of these excitatory substances causes a switch to get flipped sending the pain response spiraling upwards instead of shutting down.At its most extreme (allodynia), the nervous system can interpret even the slightest touch as eliciting pain. The pain response system at this point, as VanElzakker, puts it, has become, 'pathological'.That model of pain production has been solidly documented. VanElzakker proposes the same process causing pain sensitization in the dorsal horn is causing fatigue and other symptoms in chronic fatigue syndrome, except this time it's associated with glial cells surrounding the vagus nerve.
Glial cell release of cytokines, glutamate, free radicals, etc. in the dorsal horn of the spinal cord causes increased pain sensitivity and allodynia in susceptible individuals. At some point the constant production of these excitatory substances causes a switch to get flipped sending the pain response spiraling upwards instead of shutting down.At its most extreme (allodynia), the nervous system can interpret even the slightest touch as eliciting pain. The pain response system at this point, as VanElzakker, puts it, has become, 'pathological'.That model of pain production has been solidly documented. VanElzakker proposes the same process causing pain sensitization in the dorsal horn is causing fatigue and other symptoms in chronic fatigue syndrome, except this time it's associated with glial cells surrounding the vagus nerve.
A New Model of Fatigue
There is no reason to suspect that vagus-nerve associated glia would function any different than pain associated glia. VanElzakker
Nobody knows what a herpesvirus infection of the vagus nerve would look like, but VanElzakker doesn't see any reason it should look any different from an infection in other parts of the body.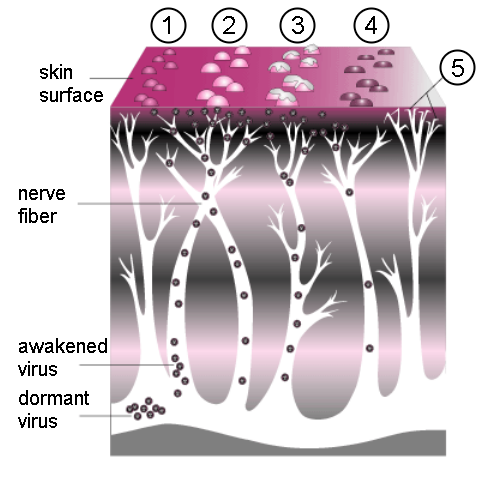 We know a herpesvirus infection of your trigeminal nerve gets you shingles and chronic pain. Researchers believe a chronic infection in the dorsal horn of your spinal cord will can get you fibromyalgia and allodynia. Would an infection of the vagus nerve get you sickness behavior and chronic fatigue syndrome?There's a good chance it might. Animal studies indicate that fatigue/flu-like symptoms go gangbusters when the vagus nerve gets infected. In fact, it's possible the flu-like symptoms associated with infections wouldn't even exist without the vagus nerve. Rodents with their vagus nerves cut don't act sick even after they've been infected with a pathogen; the fevers, fatigue, the desire for isolation - are gone.What if the vagus nerve receptors were...ceaselessly bombarded with these cytokines? The symptoms of sickness behavior would be severe and intractable.If the glial cells surrounding the vagus nerve function the same way they do in the dorsal horn, a lingering or even a 'smoldering' infection (aka Dr. Lerner's theory), could trigger the similar type of hypersensitive reaction in the vagus nerve. In this 'immune sensitization' model, it takes only very small amounts of cytokines to trigger fatigue and flu-like behavior.In fact, VanElzakker suggests chronic fatigue syndrome and fibromyalgia could both be 'glial cell diseases'.
We know a herpesvirus infection of your trigeminal nerve gets you shingles and chronic pain. Researchers believe a chronic infection in the dorsal horn of your spinal cord will can get you fibromyalgia and allodynia. Would an infection of the vagus nerve get you sickness behavior and chronic fatigue syndrome?There's a good chance it might. Animal studies indicate that fatigue/flu-like symptoms go gangbusters when the vagus nerve gets infected. In fact, it's possible the flu-like symptoms associated with infections wouldn't even exist without the vagus nerve. Rodents with their vagus nerves cut don't act sick even after they've been infected with a pathogen; the fevers, fatigue, the desire for isolation - are gone.What if the vagus nerve receptors were...ceaselessly bombarded with these cytokines? The symptoms of sickness behavior would be severe and intractable.If the glial cells surrounding the vagus nerve function the same way they do in the dorsal horn, a lingering or even a 'smoldering' infection (aka Dr. Lerner's theory), could trigger the similar type of hypersensitive reaction in the vagus nerve. In this 'immune sensitization' model, it takes only very small amounts of cytokines to trigger fatigue and flu-like behavior.In fact, VanElzakker suggests chronic fatigue syndrome and fibromyalgia could both be 'glial cell diseases'.
How to Have an Infection That Doesn't Show Up in the Blood
"Cytokines Responding to a Local Infection Stay Local" VanElzakker
If VanElzakker is right, the same group of viruses are wreaking havoc in different locations in different ME/CFS patients. The problem is it's just darn hard to get at them. You can't find them in the blood and you sure as heck can't biopsy the vagus nerve.A series of fascinating studies exploring how central nervous system infections cause chronic nerve pain may, however, illuminate what's happening in ME/CFS. First, researchers mimicked a localized nervous system infection by dropping an HIV protein known to activate glial cells into rodents' spinal cord. They found that the glial cells reared up and starting producing pro-inflammatory cytokines to take care of the intruder. Not surprisingly, the rodents looked and acted sick - the cytokines were doing their job to keep the animal down and isolated - but no trace of those cytokines could be found in their bloodstream. Only if the animal's spinal cord was sampled near where the 'infection' was it possible to find any evidence of increased cytokine levels.If VanElzakker is right, then blood cytokine levels in ME/CFS are a function of where your vagus nerve is infected. If it's infected in your abdominal area, you might find cytokines in the blood, but it might be hard to find them in your spinal fluid. If your vagus nerve is infected near your brainstem you might find cytokines in the spinal fluid, but you probably won't find them in your blood.Wherever the infection is there's a good chance you may not find cytokines in the blood at all. This isn't a completely surprising fact or even restricted to the vagus nerve infections; cytokines in mice with lung infections, for instance, showed up only when the lungs themselves were sampled.
They found that the glial cells reared up and starting producing pro-inflammatory cytokines to take care of the intruder. Not surprisingly, the rodents looked and acted sick - the cytokines were doing their job to keep the animal down and isolated - but no trace of those cytokines could be found in their bloodstream. Only if the animal's spinal cord was sampled near where the 'infection' was it possible to find any evidence of increased cytokine levels.If VanElzakker is right, then blood cytokine levels in ME/CFS are a function of where your vagus nerve is infected. If it's infected in your abdominal area, you might find cytokines in the blood, but it might be hard to find them in your spinal fluid. If your vagus nerve is infected near your brainstem you might find cytokines in the spinal fluid, but you probably won't find them in your blood.Wherever the infection is there's a good chance you may not find cytokines in the blood at all. This isn't a completely surprising fact or even restricted to the vagus nerve infections; cytokines in mice with lung infections, for instance, showed up only when the lungs themselves were sampled.
Next Steps
VanElzakker suggests animal studies to better understand infections of the vagus nerve and to ultimately to build a chronic fatigue syndrome rodent model would be helpful. Magnetic resonance imaging (MRI) may be able to detect viral lesions in central nervous system tissues. It is not yet known if PET scans can detect the activation of a different type of glial cells; the satellite glia that are in vagus nerve ganglia and paraganglia, but special PET scans might be able to be used to assess microglial activation.Cadaver studies of people who had ME/CFS definitely aren't his first choice, but they could find activated glia, inflammation and viral infections of the vagus nerve and associated structures. Finally, novel protocols should be developed to assess the vagus nerve and brainstem functioning in ME/CFS. The severely ill should be given a prominent place in future studies.

A New Treatment Approach
"Glial cell inhibitors could become standard treatment for CFS (caused by CNS vagus nerve infection)" VanElzakker
Glial Cell Inhibitors
If VE's theory is correct then glial cell inhibitors to stop the immune activation, antivirals to attack the pathogens, vagus nerve stimulation and surgical alteration of the vagus nerve might be possible treatments sometime in the future.Glial cell inhibitors have a good safety profile, have been helpful at curbing neuropathic pain and are not used much in chronic fatigue syndrome or fibromyalgia. Ibudilast (AV411/MN166), a drug used mostly in Japan, knocks down glial cell activation by inhibiting the production of a proflammatory cytokine called macrophage-migration-inhibitory factor (MIF) and TNF-a. Reduced levels of TNF-a could provide a bonus by increasing the breakdown of a excitatory neurotransmitter called glutamate that may be helping to keep your central nervous system on edge.Ibudilast is also known to have neuroprotective and vasodilative effects and is usually used to treat asthma and stroke. It's ability to suppress glial cell activation has made it useful in the treatment of neuropathic pain, and it's currently undergoing clinical trials to treat neuropathic pain in Australia. Ibudilast can also prevent viral activation of the microglia.The NIH is funding Ibudilast trials in the US to see if it's effective against drug addiction. If successful the drug could be available here for off-label use in ME/CFS in three or four years.Other general microglial inhibitors exist (minocyline, pentoxyfilline, propentfylline) but have undesirable side effects.
Ibudilast (AV411/MN166), a drug used mostly in Japan, knocks down glial cell activation by inhibiting the production of a proflammatory cytokine called macrophage-migration-inhibitory factor (MIF) and TNF-a. Reduced levels of TNF-a could provide a bonus by increasing the breakdown of a excitatory neurotransmitter called glutamate that may be helping to keep your central nervous system on edge.Ibudilast is also known to have neuroprotective and vasodilative effects and is usually used to treat asthma and stroke. It's ability to suppress glial cell activation has made it useful in the treatment of neuropathic pain, and it's currently undergoing clinical trials to treat neuropathic pain in Australia. Ibudilast can also prevent viral activation of the microglia.The NIH is funding Ibudilast trials in the US to see if it's effective against drug addiction. If successful the drug could be available here for off-label use in ME/CFS in three or four years.Other general microglial inhibitors exist (minocyline, pentoxyfilline, propentfylline) but have undesirable side effects.
Antivirals
Stopping glial cell activation may be easier than getting at the viruses themselves. Herpesviruses living in the sensory ganglia may be protected from antiviral drugs and antibodies. (One new herpesvirus drug may be coming on the market soon, however.) Alternately, viruses other than the herpesviruses could be infecting the vagus nerve.
Behavioral Therapy
VanElzakker also notes that while behavioral therapies are not curative and may only apply to a subset of patients, they can help moderate symptoms and improve quality of life in some.
Conclusion
The VNIT may be able to explain more puzzling aspects of chronic fatigue syndrome than any other. Next up we talk with Dr. VanElzakker about how he got interested in ME/CFS and what his theory may mean for this disorder.
- Follow VanElzakker on twitter here.