Large NK Cell Study Points to Autoimmunity and Inflammation in Chronic Fatigue Syndrome (ME/CFS)
The observed differences in some of the subpopulations of T and NK cells between patients and healthy controls could define a distinct immunological profile that can help in the diagnostic process of ME/CFS patients, contribute to the recognition of the disease and to the search of more specific treatments. Rivas et. Al. 2018
Problems with natural killer (NK) cell functioning have been like an anchor in the storm for immunologists interested in chronic fatigue syndrome (ME/CFS). While other immune results like cytokines have flipped and flopped all over the place, the NK cytotoxic results have been solid. Almost every study has found that when given the chance to kill infected cells, the NK cells in ME/CFS patients poop out. (The studies which have not found differences in NK cell functioning have tended not to use whole blood or used older samples - suggesting that something in the blood could be impairing NK cell functioning in ME/CFS.) The most extensive study - a year-long 2012 study involving Dr. Peterson and Griffith University in Australia - found reduced natural killer cell functioning at all time points. (Peterson has a long history of interest in natural killer cells; he was a co-author of the first study, over thirty years ago, to find deficient NK cell functioning in chronic fatigue syndrome (ME/CFS).)NK cells are important because they maintain the lines of our initial immune defense, holding the fort, so to speak, until the big guns - the T and B cells- wipe out the infection. - They also regulate the immune response.Normally our cells signal that they are infected by displaying peptide fragments from the pathogen (using MHC Class 1 molecules) on their surface. NK cells then hunt out and destroy these infected cells. However, some pathogens have learned how to prevent the cells they've infected from displaying these peptide fragments.If NK cells and other parts of the innate immune response can’t hold back the invaders, the pathogens may invade more deeply into the body, potentially causing more problems before the adaptive immune response (T and B-cells) can kick in.
The most extensive study - a year-long 2012 study involving Dr. Peterson and Griffith University in Australia - found reduced natural killer cell functioning at all time points. (Peterson has a long history of interest in natural killer cells; he was a co-author of the first study, over thirty years ago, to find deficient NK cell functioning in chronic fatigue syndrome (ME/CFS).)NK cells are important because they maintain the lines of our initial immune defense, holding the fort, so to speak, until the big guns - the T and B cells- wipe out the infection. - They also regulate the immune response.Normally our cells signal that they are infected by displaying peptide fragments from the pathogen (using MHC Class 1 molecules) on their surface. NK cells then hunt out and destroy these infected cells. However, some pathogens have learned how to prevent the cells they've infected from displaying these peptide fragments.If NK cells and other parts of the innate immune response can’t hold back the invaders, the pathogens may invade more deeply into the body, potentially causing more problems before the adaptive immune response (T and B-cells) can kick in.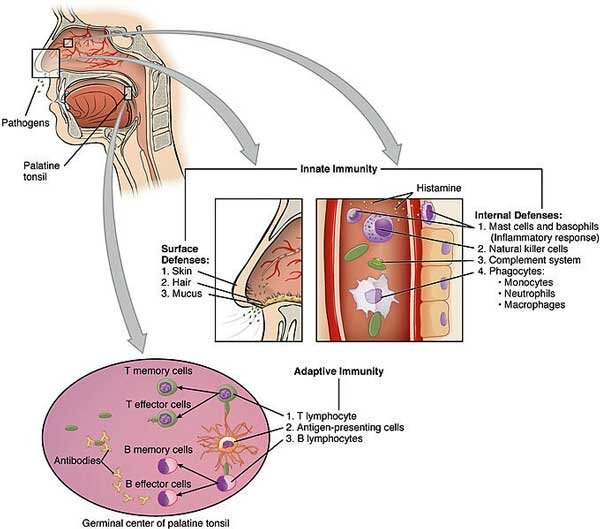 A deficient early response to pathogens would then very likely translate into more symptoms. We don’t know when the problems with NK cell killing got started in ME/CFS, but if they were in place prior to the illness or occurred early in the illness they could have played a role in the inception of ME/CFS as people who have more trouble fighting off a pathogen; i.e. people with more severe symptoms, are more likely to come down with ME/CFS.Once ME/CFS has begun, the inhibited NIK killing response could mean more trouble removing tumor and infected cells - particularly herpes virus infected cells- as people deficient in NK cells have trouble fighting off herpes viruses.NK cells, then, are vitally important, but attempts to identify issues other than cytotoxic killing abilities have been less successful. NK cells come in different types (cytotoxic and regulatory) and the balance of these subpopulations is important. Some studies have found differences in these subpopulations in ME/CFS and some have not.Many of those studies, however, have been small and used less than stringent criteria for defining ME/CFS. A Spanish group decided to rectify those problems with a more definitive study which examined NK cell populations in a larger study (n=149) with patients who met the Canadian Consensus Criteria for ME/CFS. In order to ensure they captured all factors in the blood that might be whacking NK cells, they used whole blood and analyzed it within 6 hours of collection.Then they tried to reverse engineer their results to see if a diagnostic test could be developed which simply charted which kinds of NK cells a person had. That was pretty good, but then they went further and asked if people who were worse off had different subpopulations of NK cells or more evidence of herpes virus reactivations (EBV, HMCV).
A deficient early response to pathogens would then very likely translate into more symptoms. We don’t know when the problems with NK cell killing got started in ME/CFS, but if they were in place prior to the illness or occurred early in the illness they could have played a role in the inception of ME/CFS as people who have more trouble fighting off a pathogen; i.e. people with more severe symptoms, are more likely to come down with ME/CFS.Once ME/CFS has begun, the inhibited NIK killing response could mean more trouble removing tumor and infected cells - particularly herpes virus infected cells- as people deficient in NK cells have trouble fighting off herpes viruses.NK cells, then, are vitally important, but attempts to identify issues other than cytotoxic killing abilities have been less successful. NK cells come in different types (cytotoxic and regulatory) and the balance of these subpopulations is important. Some studies have found differences in these subpopulations in ME/CFS and some have not.Many of those studies, however, have been small and used less than stringent criteria for defining ME/CFS. A Spanish group decided to rectify those problems with a more definitive study which examined NK cell populations in a larger study (n=149) with patients who met the Canadian Consensus Criteria for ME/CFS. In order to ensure they captured all factors in the blood that might be whacking NK cells, they used whole blood and analyzed it within 6 hours of collection.Then they tried to reverse engineer their results to see if a diagnostic test could be developed which simply charted which kinds of NK cells a person had. That was pretty good, but then they went further and asked if people who were worse off had different subpopulations of NK cells or more evidence of herpes virus reactivations (EBV, HMCV).
Association of T and NK Cell Phenotype With the Diagnosis of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Jose Luis Rivas,1,* Teresa Palencia,1 Guerau Fernández,2 and Milagros García1,3 Front Immunol. 2018; 9: 1028.Published online 2018 May 9. doi: 10.3389/fimmu.2018.01028
This larger, fresher (quick analysis of blood), stricter (CCC patients only) and more comprehensive study found differences where others had not – and plenty of them. This group validated - with a high degree of certainty (p = 0.0075) - previous findings of an increased subpopulation of NK cells (NK CD56++(high)) which, get this, excrete more cytokines (particularly IFN-y), possibly causing more symptoms, but which have low cytotoxic activity. Because these cells have unusually long life spans and pump out cytokines that cause more T-cell proliferation, higher numbers of them could contribute to autoimmunity and inflammation.These cells were particularly high in the group of patients whose illness began without evidence of an infection. The Spanish group suggested that activation of the stress response via the HPA axis and raised levels of catecholamines such as norepinephrine (adrenaline) could have triggered the expansion of this potentially autoimmune affecting natural killer cell subset.No differences were found, however, in the levels of several receptors (NKp46, NKp30, NKp44) that have been found elevated in some autoimmune/inflammatory conditions (Sjogren's Syndrome, Crohn's disease) or reduced in chronic infections (HIV, tuberculosis, influenza, etc.). Reduced levels of a receptor (NKG2C) were very common (p<0.0001) in ME/CFS. When this receptor, which is only found in NK cells, is activated by the presence of virally infected cells, it triggers an expansion of NK cells. Not surprisingly, NK cells become dotted with this receptor in people with chronic herpesvirus and other infections (HCMV, EBV) but ME/CFS patients’ NK cells had consistently lower levels of this receptor than did the healthy controls. The authors didn't speculate why this occurred, but it could involve lower levels of infection in ME/CFS - something Ron Davis is finding in his severely ill cohort - or a problem responding to infections that are present.That second possibility was buttressed by an inverse correlation found between a marker of infection (CD 57+) and the lower expression of a marker (NKp46) which is often reduced in herpesvirus infections. The authors suggested that the scenario found in ME/CFS (increased cd57+, lower NKp46, high NKG2C) could reflect HCMV (cytomegalovirus) reactivation.Watch Natural Killer T-cells (red) Swallow Up Antigen Presenting Dendritic Cells (green)
Reduced levels of a receptor (NKG2C) were very common (p<0.0001) in ME/CFS. When this receptor, which is only found in NK cells, is activated by the presence of virally infected cells, it triggers an expansion of NK cells. Not surprisingly, NK cells become dotted with this receptor in people with chronic herpesvirus and other infections (HCMV, EBV) but ME/CFS patients’ NK cells had consistently lower levels of this receptor than did the healthy controls. The authors didn't speculate why this occurred, but it could involve lower levels of infection in ME/CFS - something Ron Davis is finding in his severely ill cohort - or a problem responding to infections that are present.That second possibility was buttressed by an inverse correlation found between a marker of infection (CD 57+) and the lower expression of a marker (NKp46) which is often reduced in herpesvirus infections. The authors suggested that the scenario found in ME/CFS (increased cd57+, lower NKp46, high NKG2C) could reflect HCMV (cytomegalovirus) reactivation.Watch Natural Killer T-cells (red) Swallow Up Antigen Presenting Dendritic Cells (green)
Increased levels of the CD69 marker (p= 0.011) provided another suggestion that ME/CFS may be an autoimmune/inflammatory disease. This important marker, which is found on many immune cells, stimulates NK cell cytotoxic activity. More importantly, CD69 has been described as a master regulator for autoimmunity in rheumatoid arthritis (RA) through its upregulation of TGF-B - one of the very few cytokines that has usually been found increased in ME/CFS.A "descent" in T regulatory cells similar to that found in autoimmune conditions such as lupus and RA was also found. Finally, an inverted Th17/T regulatory cell ratio, which is also found in autoimmune conditions like lupus, wrapped up the autoimmune connections found in this study.Using a mathematical classification model, the group was able to correctly diagnose 70% of ME/CFS patients and healthy controls simply by using the findings from this in depth study of natural killer cell populations.
Conclusions
This large Spanish study of NK cell subpopulations found numerous irregularities in NK cell types in ME/CFS, several of which pointed to issues with autoimmunity and/or inflammation. As in other studies, this study indicates that larger is indeed better when it comes to studying ME/CFS.The study validated prior findings of an unusually large set of NK cells which produce more cytokines - conceivably causing more symptoms and immune activation - but which are less effective at killing infected cells. That finding seemed to jive with a picture of highly symptomatic ME/CFS patients who may have trouble fighting off infections.While no differences were found in the levels of receptors which can be elevated in autoimmune conditions, several other findings suggested that NK cells may be fighting off herpesvirus infections or may be involved in autoimmune/inflammatory processes in ME/CFS.Finally, using just NK cell subpopulation data, the authors were able to correctly identify 70% of patients and healthy controls, indicating that significant NK cell differences exist. All told, the study identified several natural killer irregularities that could participate in autoimmunity and dysregulate other parts of the immune system.